Why Do Starving Peoples Bellies Bloat Why Do Babies Have Big Bellies
| Kwashiorkor | |
|---|---|
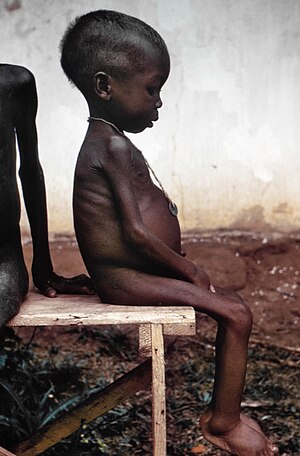 | |
| A young girl with kwashiorkor in a relief camp during the Biafra State of war | |
| Specialty | Pediatrics |
Kwashiorkor ( KWOSH-ee-OR-kor, -kər, KWASH-)[i] is a class of severe protein malnutrition characterized past edema and an enlarged liver with fatty infiltrates.[2] It is thought to be caused by sufficient calorie intake, merely with bereft protein consumption (or lack of good quality poly peptide), which distinguishes it from marasmus. Recent studies have found that a lack of antioxidant micronutrients such equally β-carotene, lycopene, other carotenoids, and vitamin C also as the presence of aflatoxins may play a part in the development of the disease.[3] However, the exact cause of kwashiorkor is all the same unknown. Inadequate food supply is correlated with occurrences of kwashiorkor; occurrences in loftier income countries are rare.[four] Information technology occurs amongst weaning children to ages of about five years old.[2]
Conditions analogous to kwashiorkor were well documented around the world throughout history.[five] However, Jamaican pediatrician Cicely Williams introduced the term in 1935, two years after she published the illness's first formal description. Williams was the first to conduct research on kwashiorkor and differentiate it from other dietary deficiencies. She was the first to suggest that this might exist a deficiency of protein.[six] [7] The name is derived from the Ga linguistic communication of coastal Ghana, translated as "the sickness the baby gets when the new baby comes" or "the disease of the deposed child", and reflecting the development of the condition in an older child who has been weaned from the breast when a younger sibling comes.[viii] Breast milk contains amino acids vital to a child's growth. In at-take chances populations, kwashiorkor may develop subsequently children are weaned from chest milk and brainstorm consuming a nutrition loftier in carbohydrates, including maize, cassava or rice.[2] [6]
Classification [edit]
Children with severe malnutrition take an increased risk of serious affliction and expiry.
Kwashiorkor is i of the main forms of childhood malnutrition living in low-income and middle-income countries. Kwashiorkor is ofttimes referred to as astringent acute malnutrition (SAM). Astringent forms of malnutritions are recognized, including stunting, marasmus, and kwashiorkor.[ix] Both kwashiorkor and marasmus fall under the umbrella of deficiencies called Protein Energy Malnutrition (PEM).[10] These diseases are oftentimes discussed together, but can be distinguished. Kwashiorkor is classified by its bereft protein consumption whereas marasmus is related to general free energy deficiency and astringent muscle wasting. Kwashiorkor is as well distinguished from marasmus past the presence of edema.There is also marasmic kwashiorkor that is the deficiency of both calories and proteins.[eleven] [three] Although they are both different types of severe acute malnutrition, there was greater consumption of antioxidants, vitamins, and minerals seen in those with kwashiorkor compared to those with marasmus.[three]
Wellcome'southward classification[12] [edit]
Wellcome classification is a arrangement for classifying protein-energy malnutrition in children based on weight for their age and based on presence of edema. Other classifications include Gomez classification and Waterlow nomenclature.[13] [xiv]
| Weight for age | With edema | Without edema | General considerations |
|---|---|---|---|
| sixty-80% | Kwashiorkor | Undernutrition |
|
| <threescore% | Marasmic kwashiorkor | Marasmus |
Signs and symptoms [edit]
The defining sign of kwashiorkor in a malnourished child is pitting edema (particularly swelling of the hands and feet). Unlike marasmus, where the liver and other essential organs are reduced in size, kwashiorkor is characterized past "an enlarged fatty liver, fibrosis, and dysfunction of several organs (such as the liver, kidneys, and nervous organisation)".[3] Other signs include a distended abdomen, thinning of hair, loss of teeth, skin or hair depigmentation, and dermatitis. Children with kwashiorkor ofttimes develop irritability and anorexia. Mostly, the disease can exist treated by adding protein to the diet; however, it can accept a long-term impact on a kid'southward physical and mental evolution, and in severe cases may pb to death.[ citation needed ]
In dry out climates, marasmus is the more frequent affliction associated with malnutrition. Another malnutrition syndrome includes cachexia, although it is often acquired by underlying illnesses. These are important considerations in the treatment of individuals with kwashiorkor.[ citation needed ]
Causes [edit]
The precise etiology of kwashiorkor remains unclear.[15] [sixteen] [17] [eighteen] Several hypotheses have been proposed that are associated with and explain some, but not all aspects of the pathophysiology of kwashiorkor. They include, merely are not limited to poly peptide deficiency causing hypoalbuminemia, amino acrid deficiency, oxidative stress, and gut microbiome changes.[xv] [xviii] [nineteen]
Depression protein intake [edit]

Disability-adapted life years per 100,000 inhabitants for poly peptide–free energy malnutrition in 2002.[20]
no data
fewer than 10
10–100
100–200
200–300
300–400
400–500
500–600
600–700
700–800
800–1000
thousand–1350
more than than 1350
Kwashiorkor is a severe form of malnutrition associated with a deficiency in dietary protein.[two] The extreme lack of protein causes an osmotic imbalance in the gastrointestinal system causing swelling of the gut diagnosed equally an edema or retention of h2o.[vii]
Extreme fluid retention observed in individuals suffering from kwashiorkor is a direct event of irregularities in the lymphatic organization and an indication of capillary exchange. The lymphatic system serves three major purposes: fluid recovery, immunity, and lipid absorption. Victims of kwashiorkor commonly exhibit reduced ability to recover fluids, allowed system failure, and depression lipid absorption, all of which result from a state of astringent undernourishment. Fluid recovery in the lymphatic system is accomplished by re-absorption of water and proteins which are so returned to the claret. Compromised fluid recovery results in the characteristic abdomen distension observed in highly malnourished children.[21]
Capillary exchange betwixt the lymphatic organization and the bloodstream is stunted due to the inability of the body to effectively overcome the hydrostatic pressure level gradient. Proteins, mainly albumin, are responsible for creating the colloid osmotic pressure (COP) observed in the blood and tissue fluids. The difference in the COP of the blood and tissue is called the oncotic force per unit area. The oncotic pressure is in straight opposition with the hydrostatic pressure and tends to draw water back into the capillary past osmosis. All the same, due to the lack of proteins, no substantial pressure level gradient tin be established to draw fluids from the tissue back into the blood stream. This results in the pooling of fluids, causing the swelling and distention of the belly.[22]
The low protein intake leads to some specific signs: edema of the hands and feet, irritability, anorexia, a desquamative rash, hair discolouration, and a big fat liver. The typical swollen abdomen is due to ii causes: ascites considering of hypoalbuminemia (depression oncotic pressure), and enlarged fatty liver.[23]
Ignorance of nutrition can be a crusade. A case was described where parents who fed their child cassava failed to recognize malnutrition because of the edema acquired by the syndrome and believed the child was well-nourished despite the lack of dietary poly peptide.[24]
Poly peptide should be supplied simply for anabolic purposes. The catabolic needs should be satisfied with carbohydrate and fat. Poly peptide catabolism involves the urea cycle, which is located in the liver and can hands overwhelm the capacity of an already damaged organ. The resulting liver failure can be fatal. This ways in individuals suffering from kwashiorkor, protein must be introduced back into the diet gradually. Clinical solutions include weaning the affected with milk products and increasing the intake of proteinaceous material progressively to daily recommended amounts.[ citation needed ]
Aflatoxins [edit]
Contempo studies have attempted to pinpoint a relationship between kwashiorkor and high levels of aflatoxins. Aflatoxins are naturally occurring toxins produced by the mold Aspergillus flavus, a fungus plant in areas with hot and humid climates.[25] These toxins tend to grow and can be found in agricultural crops such as millet, maize, and rice.[25] An analysis found that the presence of aflatoxins was found more often and in college concentrations in individuals with kwashiorkor when compared to individuals with marasmus (another form of severe astute malnutrition).[26] [27] In item, biological samples showed greater levels of aflatoxins in the brain, heart, kidney, liver, lungs, serum, stool, and urine.[26] Aflatoxins were not found in liver samples of individuals with marasmus.[26] It has been known that the liver organ is the main target of aflatoxins and chronic toxicity can consequence in immunosuppressive and carcinogenic furnishings.[26] However, there is currently conflicting testify to pinpoint a connection between kwashiorkor and aflatoxins. Studies have shown that not all children with kwashiorkor present with detectable aflatoxin levels.[iii] It has also been proposed that damage washed past aflatoxins may be due to glutathione depletion (some other proposed mechanism of the illness) in children with kwashiorkor.[3]
Mechanisms [edit]
Peripheral edema and hypoalbuminemia [edit]
Kwashiorkor is a form of protein deficiency, which can consequence in both osmotic imbalances and irregularities in the lymphatic organization.[three]
Kwashiorkor is most notable for peripheral edema. The presence of edema in kwashiorkor is correlated with very depression albumin concentration (hypoalbuminemia). Edema results from a loss of fluid balance between the hydrostatic and oncotic pressures beyond the capillary blood vessel walls[2] due to the lack of protein which affects the torso's ability to draw fluid from the tissues into the bloodstream. Low albumin concentration influences negatively the force of oncotic force per unit area. Failure leads to the fluid buildup in the abdomen, resulting in edema and belly distension.[iii]
Furthermore, the release of antidiuretic hormone is stimulated past hypovolemia, also leading to the evolution of peripheral edema. Plasma renin is also stimulated, promoting sodium retention.[2]
It is important to distinguish the pathophysiology of marasmus and kwashiorkor when information technology comes to treating malnourished children who may have hypovolemic shock that is cause by an acute loss of common salt and h2o.[xvi] Children with astringent albumin deficiency struggle physiologically to maintain their blood volume.[16]
Low glutathione levels [edit]
Kwashiorkor is also marked by depression glutathione levels. Glutathione is used in many of the body processes on a molecule level.[28]
It is believed to be related to high oxidant levels unremarkably seen in people who suffer from starvation and rarely in chronic inflammation.[2] Glutathione serves vital functions including direction of oxidative stress which is an imbalance that plays a cardinal role in the pathogenesis of many diseases.
Cysteine is an essential amino acid that acts as the limiting amino acid for glutathione synthesis in humans. Factors that stimulate cysteine uptake by cells will increase glutathione levels and prevent glutathione deficiency in humans under various conditions including poly peptide malnutrition.[28]
Show indicates that dietary amino acids balance has an important effect on poly peptide nutrition and therefore on glutathione homeostasis.[29]
Others [edit]
A proposed experimental theory suggests that alterations in the microbiome/virone contributes to edematous malnutrition, simply further studies are required to understand the mechanism.[2]
Diagnosis [edit]
Kwashiorkor, or edematous malnutrition, like many other malnutrition diseases, is indirectly assessed using anthropometry.[9] Kwashiorkor is a subtype of astringent acute malnutrition (SAM) characterized past bilateral peripheral pitting edema. According to the World Wellness Organisation, the SAM diagnosis parameters are a "mid-upper arm circumference (MUAC) of < 115 mm, weight-for-height/length Z-score (WHZ) of < -3Z and nutritional edema or whatever combination of these parameters."[thirty] [2] [31] Boosted clinical findings on physical test include marked muscle atrophy, abdominal amplification, dermatitis, and hepatomegaly.[2] [32]
WHO criteria for clinical assessment of malnutrition are based on the degree of wasting (MUAC), stunting (weight-for-height Z-score), and the presence of edema (mild to severe).[33]
Screening [edit]
Considering information technology can exist hard to measure weight-for-elevation Z scores (WHZ) frequently, screening is performed using mid-upper arm circumference (MUAC) < 115 mm.[9] To properly screen for severe malnutrition in children, MUAC measurements should be washed every calendar month to reduce the adventure of complications.[nine] Additionally, getting a better sense of what they eat, how oft they eat, and any issues they may have with eating, may give more insight on their nutrition and what changes may demand to be made to improve it.[34]
Prevention [edit]
Equally for the prevention of childhood malnutrition, there needs to exist public health changes such as improving agronomics and improving access to healthcare to effectively reduce the rates of malnutrition in children. By educating individuals of childbearing age on proper nutrition and health during and later pregnancy, they can provide their children with the advisable nutrients from a young age. By ensuring they are equipped with the proper education and resources, caretakers and infants are in better health, ultimately preventing childhood malnutrition.[nine]
Considering edema can hide decreased muscle mass, information technology can be hard to diagnose kwashiorkor in immature children; however, if cases are overlooked, children become more than susceptible to infections and tin can ultimately pb to morbidity and mortality.[35] To prevent this from happening, parents can be educated on proper nutrition and the importance of breastfeeding infants to ensure they receive all the nutrients they need.[35]
A diet rich in carbohydrates, fats that make upwards x% of the total caloric needs, and proteins that make upwardly 15% of the caloric needs can forestall kwashiorkor.
Proteins can be found in the following foods
- Seafood
- Peas
- Nuts
- Seeds
- Eggs
- Lean meat
- Beans[3]
Treatment [edit]
WHO guidelines outline 10 general principles for the inpatient management of severely malnourished children.[33] [36]
- Treat/prevent hypoglycemia
- Treat/foreclose hypothermia
- Care for/prevent dehydration
- Correct electrolyte imbalance
- Treat/prevent infection
- Correct micronutrient deficiencies
- Start cautious feeding
- Achieve catch-up growth
- Provide sensory stimulation and emotional support
- Prepare for follow-up later on recovery
Both clinical subtypes of severe acute malnutrition (kwashiorkor and marasmus) are treated similarly.[18] [33] Upon initial treatment, children with kwashiorkor may feel weight loss as their edema resolves.[37] Therefore, after concerns of refeeding syndrome have passed, children may crave 120-140% of their estimated caloric needs in order to achieve catch-up growth.[37]
The cause, type, and severity of malnutrition determines what type of treatment would be near advisable.[34] For main acute malnutrition, children with no complications are treated at home and are encouraged to either continue breastfeeding (for infants) or starting time using set-to-use therapeutic foods (for children).[34] For secondary acute malnutrition, the underlying cause needs to be identified to accordingly care for children. Only after the primary disease is determined can an advisable dietary program be fabricated, as fluid, vitamins, and macronutrients may need to be considered to non exacerbate the cause of the malnutrition.[34]
Ready-to-use therapeutic foods (RUTFs) and F-75 and F-100 milks were created to provide appropriate nutrition and caloric intake to those experiencing malnutrition. F-75 milk would exist ideal when trying to reintroduce food into a malnourished person, and F-100 milk would exist used to aid in weight proceeds. While RUTFs and F-100 milk were made to accept the same nutritional value, RUTFs are beneficial as they are dehydrated and exercise not crave much training.[9]
Prognosis [edit]
Kwashiorkor is associated with a high risk of mortality and long-term complications. Handling under the guidelines of the World Health Organization has proven to reduce this mortality take a chance and afflicted children tend to recover faster than children with other severe malnutrition diseases. However, concrete and intellectual capabilities are not fully restored. Growth stunting and chronic disruption of microbiota are commonly observed after recovery.[three]
A high gamble of decease is identified by a brachial perimeter < 11 cm or by a weight-for-historic period threshold < −3 z-scores beneath the median of the WHO kid growth standards. In practice, malnourished children with edema are suffering from potentially life-threatening severe malnutrition.[38]
Epidemiology [edit]
Kwashiorkor is rare in high income countries. It is by and large observed in low-income and eye income nations and regions such every bit Southeast Asia, Central America, Congo, Ethiopia, Puerto Rico, Jamaica, South Africa, and Uganda, where poverty is prominent.[3] Occurrences of severe malnutrition also tend to trend higher under weather condition of nutrient insecurity, higher prevalence of infectious diseases, lack of admission to advisable care, and poor living situations with inadequate sanitation.[nine] Communities experiencing famine are affected the well-nigh especially during the rainy season. Prevalence varies, but it affects children of either sexual practice ordinarily under five years sometime.[3] [10] "Globally, kwashiorkor indirected deemed for 53% of deaths among children under five betwixt 2000 and 2003 when associated with other common childhood diseases like acute respiratory infections, malaria, measles, HIV/AIDS and other causes of perinatal deaths."[10]
When compared to marasmus in developing countries, kwashiorkor has a lower prevalence, "0.ii%-1.half-dozen% for kwashiorkor and 1.2%-vi.8% for marasmus."[3] Factors such as "diet, geographical locations, climate and aflatoxin exposure" are associated with the difference in prevalence for kwashiorkor and marasmus.[three]
History [edit]
It is likely that kwashiorkor was commonly seen around the world long before 1933, when Cicely Williams published research which took the Ga name for the affliction. In that location were already many names for the illness which referenced the abeyance of breastfeeding, or the consumption of diets which were too high in starch. However, Williams was the first to suggest that this might be a deficiency of protein. [7] [5] Despite publishing in 1933, it was merely in 1949 that the World Health Arrangement officially recognized kwashiorkor equally a public health business concern.[2] This period also correlated with the promotion of infant formula, oftentimes by European colonial powers. The substitution of breastmilk for formula contributed significantly to the increasing visibility of kwashiorkor throughout the twentieth century. Cicely Williams afterwards described the promotion of formula as "the virtually criminal form of sedition, and that those deaths should be regarded as murder." These arguments underpinned the 1970s Nestlé boycott.[v]
Effects on pharmacokinetics [edit]
Those experiencing poverty-related infectious diseases (PRDs) such every bit malaria and tuberculosis are also likely to be malnourished.[39] Malnutrition can impact the pharmacokinetics of various drugs used to care for PRDs by changing a drug'south bioavailability, distribution, and elimination.[39] To optimize handling of those diseases, at that place needs to exist more inquiry into how astringent malnutrition, specifically kwashiorkor, can affect handling response.[39]
Research directions [edit]
Current research and recommendations to manage astringent acute malnutrition (SAM), such equally kwashiorkor, in children are largely based on skilful opinions. Merely one-3rd of the WHO guidelines for management of SAM are based on epidemiological and clinical research. Further studies are needed in lodge to "meliorate treatment outcomes in the large number of children with SAM."[40]
See as well [edit]
- Anemia
- Emaciation
- Starvation
- Marasmus
- Protein poisoning
References [edit]
- ^ Wells, John C. (2008). Longman Pronunciation Dictionary (3rd ed.). Longman. ISBN978-1-4058-8118-0.
- ^ a b c d east f g h i j one thousand Benjamin, Onecia; Lappin, Sarah L. (2022). "Kwashiorkor". StatPearls. StatPearls Publishing. PMID 29939653. NBK507876.
- ^ a b c d east f g h i j k fifty m n Pham, Thi-Phuong-Thao; Alou, Maryam Tidjani; Golden, Michael H.; Million, Matthieu; Raoult, Didier (January 2021). "Deviation between kwashiorkor and marasmus: Comparative meta-analysis of pathogenic characteristics and implications for treatment". Microbial Pathogenesis. 150: 104702. doi:10.1016/j.micpath.2020.104702. PMID 33359074. S2CID 229694345.
- ^ Liu T, Howard RM, Mancini AJ, Weston WL, Paller AS, Drolet BA, et al. (2001). "Kwashiorkor in the United States: fad diets, perceived and true milk allergy, and nutritional ignorance". Archives of Dermatology. 137 (five): 630–6. PMID 11346341. [ permanent dead link ]
- ^ a b c Nott, John (May 2021). "'No one may starve in the British Empire': Kwashiorkor, Poly peptide and the Politics of Nutrition Between Britain and Africa". Social History of Medicine. 34 (2): 553–576. doi:ten.1093/shm/hkz107. PMC8162845. PMID 34084092.
- ^ a b Williams CD (1983) [1933]. "Fifty years ago. Archives of Diseases in Childhood 1933. A nutritional disease of babyhood associated with a maize diet". Archives of Disease in Childhood. 58 (7): 550–lx. doi:10.1136/adc.58.7.550. PMC1628206. PMID 6347092.
- ^ a b c Williams CD, Oxon BM, Lond H (1935). "Kwashiorkor: a nutritional disease of children associated with a maize diet. 1935". Bulletin of the World Wellness Arrangement. 81 (12): 912–3. doi:10.1016/S0140-6736(00)94666-X. PMC2572388. PMID 14997245. Reprint: Williams CD, Oxon BM, Lond H (2003). "Kwashiorkor: a nutritional illness of children associated with a maize diet. 1935". Bulletin of the Earth Health Organisation. 81 (12): 912–3. doi:10.1016/S0140-6736(00)94666-Ten. PMC2572388. PMID 14997245.
- ^ Stanton, J. (2001). "Listening to the Ga: Cicely Williams' Discovery of Kwashiorkor on the Gold Coast" (PDF). Women and Modern Medicine. Clio Medica. Vol. 61. pp. 149–171. doi:10.1163/9789004333390_008. ISBN978-ninety-04-33339-0. PMID 11603151.
- ^ a b c d due east f thou Bhutta, Zulfiqar A.; Berkley, James A.; Bandsma, Robert H. J.; Kerac, Marko; Trehan, Indi; Briend, André (21 December 2017). "Severe babyhood malnutrition". Nature Reviews Disease Primers. three (1): 17067. doi:10.1038/nrdp.2017.67. PMC7004825. PMID 28933421.
- ^ a b c Odigwe, Chibuzo C; Smedslund, Geir; Ejemot-Nwadiaro, Regina I; Anyanechi, Chiedozie C; Krawinkel, Michael B (14 April 2010). "Supplementary vitamin E, selenium, cysteine and riboflavin for preventing kwashiorkor in preschool children in developing countries". Cochrane Database of Systematic Reviews (iv): CD008147. doi:10.1002/14651858.CD008147.pub2. PMC6599860. PMID 20393967.
- ^ "Malnutrition (Kwashiorkor and Marasmus) — Symptoms and Handling". The Lecturio Online Medical Library. 2017. Retrieved 27 July 2021.
- ^ "Poly peptide energy malnutrition classification - wikidoc". world wide web.wikidoc.org . Retrieved 29 July 2021.
- ^ Bough, David A., ed. (29 Jan 2009). "Wellcome nomenclature". A Dictionary of Food and Nutrition. OUP Oxford. ISBN978-0-xix-157975-ii.
- ^ Gernaat, H.; Voorhoeve, HW (1 April 2000). "A new classification of acute protein-energy malnutrition". Journal of Tropical Pediatrics. 46 (2): 97–106. doi:10.1093/tropej/46.two.97. PMID 10822936.
- ^ a b Briend A (2014). "Kwashiorkor: still an enigma – the search must go on" (PDF). Emergency Nutrition Network . Retrieved ii August 2019.
- ^ a b c One thousand. Coulthard, Malcolm (13 May 2015). "Oedema in kwashiorkor is caused by hypoalbuminaemia". Paediatrics and International Kid Wellness. 35 (ii): 83–89. doi:10.1179/2046905514Y.0000000154. PMC4462841. PMID 25223408.
- ^ Pham, Thi-Phuong-Thao; Tidjani Alou, Maryam; Bachar, Dipankar; Levasseur, Anthony; Brah, Souleymane; Alhousseini, Daouda; Sokhna, Cheikh; Diallo, Aldiouma; Wieringa, Frank; Million, Matthieu; Raoult, Didier (December 2019). "Gut Microbiota Alteration is Characterized by a Proteobacteria and Fusobacteria Bloom in Kwashiorkor and a Bacteroidetes Paucity in Marasmus". Scientific Reports. 9 (1): 9084. Bibcode:2019NatSR...9.9084P. doi:ten.1038/s41598-019-45611-3. PMC6591176. PMID 31235833.
- ^ a b c Smith, Michelle I.; Yatsunenko, Tanya; Manary, Mark J.; Trehan, Indi; Mkakosya, Rajhab; Cheng, Jiye; Kau, Andrew L.; Rich, Stephen South.; Concannon, Patrick; Mychaleckyj, Josyf C.; Liu, Jie; Houpt, Eric; Li, Jia V.; Holmes, Elaine; Nicholson, Jeremy; Knights, Dan; Ursell, Luke M.; Knight, Rob; Gordon, Jeffrey I. (February 2013). "Gut Microbiomes of Malawian Twin Pairs Discordant for Kwashiorkor". Scientific discipline. 339 (6119): 548–554. Bibcode:2013Sci...339..548S. doi:10.1126/scientific discipline.1229000. PMC3667500. PMID 23363771.
- ^ Velly H, Britton RA, Preidis GA (2017). "Mechanisms of cross-talk between the diet, the intestinal microbiome, and the undernourished host". Gut Microbes. eight (2): 98–112. doi:x.1080/19490976.2016.1267888. PMC5390823. PMID 27918230.
- ^ "Mortality and Burden of Illness Estimates for WHO Member States in 2002" (xls). Globe Health Organization. 2002.
- ^ "Nova et Vetera". The British Medical Journal. ii (4673): 284. 1950. doi:10.1136/bmj.2.4673.267. S2CID 220181068.
- ^ Saladin K (2012). Anatomy and Physiology (6th ed.). New York: McGraw Hill. pp. 766–767, 809–811. ISBN978-0-07-337825-1.
- ^ Tierney EP, Sage RJ, Shwayder T (2010). "Kwashiorkor from a severe dietary brake in an eight-calendar month infant in suburban Detroit, Michigan: example report and review of the literature". International Journal of Dermatology. 49 (5): 500–6. doi:10.1111/j.1365-4632.2010.04253.10. PMID 20534082. S2CID 13050691.
- ^ "Malnutrition in Third Earth Countries". world wide web.religion-online.org. Archived from the original on 19 September 2015. Retrieved 2 March 2017.
- ^ a b Kumar, Pradeep; Mahato, Dipendra K.; Kamle, Madhu; Mohanta, Tapan K.; Kang, Sang G. (17 January 2017). "Aflatoxins: A Global Concern for Nutrient Safe, Human Health and Their Management". Frontiers in Microbiology. 07: 2170. doi:10.3389/fmicb.2016.02170. PMC5240007. PMID 28144235.
- ^ a b c d Soriano, Jose M.; Rubini, Ana; Morales-Suarez-Varela, María; Merino-Torres, Juan F.; Silvestre, Dolores (October 2020). "Aflatoxins in organs and biological samples from children affected by kwashiorkor, marasmus and marasmic-kwashiorkor: A scoping review". Toxicon. 185: 174–183. doi:10.1016/j.toxicon.2020.07.010. PMID 32693007. S2CID 220698925.
- ^ Watson, Sinead; Gong, Yun Yun; Routledge, Michael (xv July 2015). "Interventions Targeting Kid Undernutrition in Developing Countries May Be Undermined by Dietary Exposure to Aflatoxin" (PDF). Disquisitional Reviews in Food Scientific discipline and Nutrition. 57 (nine): 1963–1975. doi:ten.1080/10408398.2015.1040869. PMID 26176888. S2CID 24089209.
- ^ a b Wu, Fang, Yang, Lupton, Turner, Guoyo, Yun-Zhong, Sheng, Joanne R, Nancy D. (2004). "Glutathione Metabolism and Its Implications for Health". The Periodical of Diet. 134 (3): 489–492. doi:10.1093/jn/134.iii.489. PMID 14988435. Retrieved 29 July 2021.
{{cite periodical}}: CS1 maint: multiple names: authors list (link) - ^ Gould, Rebecca L.; Pazdro, Robert (11 May 2019). "Affect of Supplementary Amino Acids, Micronutrients, and Overall Diet on Glutathione Homeostasis". Nutrients. 11 (5): 1056. doi:10.3390/nu11051056. PMC6566166. PMID 31083508.
- ^ Roberfroid, Dominique; Hammami, Naïma; Mehta, Pankti; Lachat, Carl; Verstraeten, Roosmarijn; Weise Prinzo, Zita; Huybregts, Lieven; Kolsteren, Patrick (2013). Management of oedematous malnutrition in infants and children aged >6 months: a systematic review of the evidence. CiteSeerXten.i.1.655.6549. hdl:1854/LU-5700347.
- ^ Grellety, Emmanuel; Gilded, Michael H. (December 2018). "Severely malnourished children with a low weight-for-height accept similar mortality to those with a low mid-upper-arm-circumference: II. Systematic literature review and meta-assay". Nutrition Journal. 17 (1): eighty. doi:10.1186/s12937-018-0383-5. PMC6138903. PMID 30217196.
- ^ Heilskov, Due south.; Rytter, Chiliad.J.H.; Vestergaard, C.; Briend, A.; Babirekere, E.; Deleuran, M.S. (August 2014). "Dermatosis in children with oedematous malnutrition (Kwashiorkor): a review of the literature". Journal of the European Academy of Dermatology and Venereology. 28 (eight): 995–1001. doi:10.1111/jdv.12452. PMID 24661336. S2CID 24731334.
- ^ a b c Guideline: updates on the management of severe astute malnutrition in infants and children. World Health System. 2013. hdl:10665/95584. ISBN978-92-4-150632-eight. [ folio needed ]
- ^ a b c d Dipasquale, Valeria; Cucinotta, Ugo; Romano, Claudio (12 August 2020). "Acute Malnutrition in Children: Pathophysiology, Clinical Furnishings and Treatment". Nutrients. 12 (eight): 2413. doi:10.3390/nu12082413. PMC7469063. PMID 32806622.
- ^ a b Kamaruzaman, NA; Jamani, NA; Said, AH (6 July 2020). "An infant with kwashiorkor: The forgotten disease". Malaysian Family unit Physician. 15 (ii): 46–49. PMC7430309. PMID 32843945.
- ^ Ashworth A (2003). "Guidelines for the inpatient treatment of severely malnourished children" (PDF). WHO. Archived from the original (PDF) on 27 March 2006.
- ^ a b Grover, Zubin; Ee, Looi C. (Oct 2009). "Poly peptide Free energy Malnutrition". Pediatric Clinics of N America. 56 (5): 1055–1068. doi:ten.1016/j.pcl.2009.07.001. PMID 19931063.
- ^ "Direction of moderate malnutrition in under-v children past the health sector" (PDF).
- ^ a b c Verrest, Luka; Wilthagen, Erica A.; Beijnen, Jos H.; Huitema, Alwin D. R.; Dorlo, Thomas P. C. (September 2021). "Influence of Malnutrition on the Pharmacokinetics of Drugs Used in the Handling of Poverty-Related Diseases: A Systematic Review". Clinical Pharmacokinetics. threescore (9): 1149–1169. doi:10.1007/s40262-021-01031-z. PMC8545752. PMID 34060020. S2CID 235259789.
- ^ Kulkarni, Bharati; Mamidi, RajaSriswan (2019). "Nutrition rehabilitation of children with severe acute malnutrition: Revisiting studies undertaken by the National Institute of Nutrition". Indian Journal of Medical Inquiry. 150 (2): 139–152. doi:10.4103/ijmr.IJMR_1905_18. PMC6829782. PMID 31670269.
External links [edit]
- Picot, J; Hartwell, D; Harris, P; Mendes, D; Clegg, A J; Takeda, A (2012). "The effectiveness of interventions to treat severe acute malnutrition in young children: a systematic review". Health Technology Assessment. 16 (19). doi:10.3310/hta16190. PMC4781582. PMID 22480797. NBK98566.
-
 Media related to Kwashiorkor at Wikimedia Commons
Media related to Kwashiorkor at Wikimedia Commons
Source: https://en.wikipedia.org/wiki/Kwashiorkor
0 Response to "Why Do Starving Peoples Bellies Bloat Why Do Babies Have Big Bellies"
Post a Comment